
UgandaToday: Uganda’s Deadliest Hour: A Chronicle of Crisis, Disease, and Survival
Uganda in 2025 finds itself standing in the furnace of overlapping catastrophes that cut across disease, death, insecurity, and institutional fragility, weaving a tapestry of mortality that is as statistical as it is human.
Sudan Virus Disease Outbreak
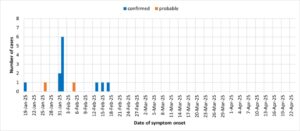
The outbreak of Sudan virus disease (SVD)—a lethal cousin of Ebola—first declared on 30 January 2025, epitomizes the fragility of a health system already staggering under multiple burdens.
By 5 March, official counts documented 14 cases (12 confirmed, 2 probable) with 4 deaths, giving a case fatality ratio of roughly 29%. Though lower than the notorious Ebola Zaire strain, the figure carried the weight of terror in a nation where hospitals are thinly stretched and fear spreads faster than microbes.
Surveillance mapped the cases to Kampala, Wakiso, Mbale, and Ntoroko, revealing how a pathogen can traverse districts with ease in a nation of over 48 million citizens, many living in dense urban settlements. Nearly 200 contacts were listed for monitoring, each a potential vector for community transmission.
While the Ministry of Health declared the outbreak over by 26 April 2025—after 42 days without new infections—the crisis laid bare the glaring absence of a licensed vaccine for the Sudan strain and the danger of reactive rather than preventive response. The specter of Ebola remains ever-present, especially in a nation bordering the Democratic Republic of Congo, where zoonotic spillovers occur frequently. Every lull in cases is not peace but an intermission.

Preventable Diseases: Uganda’s Silent Killers
Ebola, however, is only the tip of Uganda’s mortality iceberg. The larger, quieter killers are preventable diseases that stalk homes, clinics, and maternity wards daily, leaving behind invisible graves.
Facility data from the 2023/2024 financial year reads like a ledger of neglect:
-
9.4% of all recorded deaths were linked to neonatal conditions—babies who never breathed, who gasped and failed, who succumbed to sepsis or asphyxia within hours of birth. This translated to roughly 4,208 facility deaths. The true toll is higher, as many rural mothers still deliver outside hospitals without incubators, oxygen, or skilled midwives.
-
Pneumonia claimed 3,698 lives.
-
Malaria, despite known treatment and prevention strategies, killed 2,917.
Together, these three conditions accounted for more than 10,000 facility-recorded deaths. The true number is likely double when home deaths are factored in, especially in rural Uganda.
Here lies the grim truth: Uganda’s deadliest realities are not always sensational outbreaks, but the grinding repetition of common diseases left unmastered.
Refugee Health Burdens
Overlaying this epidemiological crisis is the challenge of refugee health. Uganda hosts nearly 1.6 million displaced persons, the highest number in Africa—mostly from South Sudan and the Democratic Republic of Congo.
Settlements in western and northern Uganda have become epicentres for measles and rubella outbreaks. In April 2025, health officials confirmed at least nine measles cases among refugee children, some fatal, prompting emergency vaccination drives. Yet low immunization coverage—caused by displacement, poverty, and cultural barriers—creates tinderboxes for epidemics.
When combined with chronic malnutrition, poor sanitation, and high fertility rates, refugee settlements become pressure cookers where mortality multiplies. Uganda’s humanitarian compassion has brought responsibility, but insufficient resources have converted hospitality into vulnerability.
Violence and Insecurity
The crisis of mortality in Uganda is not medical alone. Violence and insecurity deepen the wounds, creating death both directly and indirectly.
Police records from 2024 reveal 188 murders by shooting nationwide, with Moroto District in Karamoja registering the highest share—9 killings. These figures reflect escalating armed criminality, cattle rustling, and revenge killings.
Karamoja, with its history of raiding and porous borders, has become a theatre of bloodshed. Violence here not only claims lives instantly but also paralyzes social systems:
-
Families flee.
-
Clinics are abandoned.
-
Teachers leave schools.
-
Ambulances cannot move safely at night.
The hidden death toll includes children dying of malnutrition in displacement, patients perishing because roads are unsafe, and mothers bleeding to death without timely medical access. Violence magnifies disease, and disease magnifies violence—together deepening Uganda’s mortality ledger.
The Government Response: “24.2-Hours Initiative”
Amid this grim backdrop, the government launched the “24.2-hours initiative” on 25 April 2025 as a potential game-changer against malaria.
The goal is mathematically precise:
-
Treat uncomplicated malaria within 24 hours.
-
Treat severe malaria within 2 hours.
Projections suggest that, if fully resourced, this programme could cut malaria deaths by 50% and reduce severe cases by 80%—saving 1,400 lives annually and preventing 500,000 hospitalisations.
But the paradox remains: solutions exist, yet their impact depends on scale, funding, and political will. Uganda spends only USD 18 per capita annually on health—far below the USD 86 minimum recommended by the World Health Organization.
A Convergence of Crises
Uganda’s deadliest hour is not defined by a single catastrophe but by the convergence of many:
-
A lethal virus emerging and receding.
-
Thousands of infants lost to fragile health systems.
-
Refugee settlements struggling with outbreaks.
-
Armed raiders leaving villages silent.
-
Systemic underfunding that ties the hands of health workers.
Each statistic is not just a number but a life ended prematurely, a family broken, a community wounded.
Unless Uganda radically expands health investment, fortifies disease surveillance, secures volatile regions, and tackles root causes of poverty and instability, the cycle will continue.
History shows that Uganda has survived civil wars, HIV, and Ebola shocks. But survival without transformation is simply endurance. The convergence of crises in 2025 demands not endurance but a new social contract—one that treats life as sacred, statistics as urgent, and mortality not as fate but as a solvable equation.
Hashtags
#UgandaToday #HealthCrisis #Epidemics #RefugeeHealth #PublicHealth #Malaria #Ebola #KaramojaCrisis #OperaNewsFeeds #PhoenixNewsFeeds
Publisher


